
Tips: FAQs
This article is part of WAMSS's MD2 Rotations Guide. Start with page one to check out our other useful tips in this series.
Note: The advice shown here may not reflect current Department of Health or UWA School of Medicine policies, particularly with changing public health developments. If you are ever unsure, you should always seek clarification from the UWA Medical School.
Have you gone through UWA MD2? We value your advice. Notice any errors? Get in touch at [email protected]
This document is not an official WAMSS policy document. For any questions or for more information, please contact [email protected]
Contributors: Britt Suann, Jun-Ting Yeung
Last edited: 2021-08-14
This document is not an official WAMSS policy document. For any questions or for more information, please contact [email protected]
Last edited: 2021-08-14
WAMSS Clinical Prep: 7 Key Tips
-
Don’t be late – being on time makes a good impression
-
Introduce yourself to staff
-
Be helpful – collect files before ward rounds, have the obs ready
-
Get a nerd box
-
Ask questions – don’t be afraid
-
Don’t leave at 10:00am because you love Robin’s Pathology
-
Talk to patients – practice your histories and examination
What are some things that I might be asked to do?
- Find the patient's file
- Examine a patient - learn abbreviated CVS, Resp, abdo exams
- What are the patient's observations? Have they pooped today? What are they on for pain relief?
- Write notes for Mr Jones
- Take bloods or put a cannula in - always ask for help!
What am I expected to know?
- Try your best - there’s no expectation that you know anything, and it’s more surprising if you do! Your expectations as a 1st year clinical student is very reasonable, so make the most of this time to learn from your seniors and slowly mould yourself into the doctor you once envisioned
- Towards the end of MD2, you are expected to know history and examination findings for different presentations. This is what your exam will be on.
How to get a head-start on your learning?
- Try and see patients WITHOUT knowing their diagnosis; MD2 is mainly about getting comfortable with taking a good history and exam
- Contrary to popular belief, exams aren’t entirely core conditions. General hospital sense (i.e. how to consent a patient for surgery, how to manage an acutely manic patient, fluids) are all examinable content
- Specific things to learn: Early days I had no idea about what each of the blood tests meant but it's you’ll get better in time – maybe prepare by looking at the different things you can order. Main ones are FBC, UEC, LFTs, TFTs, Group and Hold for surg, Phosphate, Calcium.
- Look up some common conditions from your specialty so you know what is going on and you can ask useful questions. For example, a cardiologist isn’t going to explain to you what a STEMI is, but they may help you answer questions about an ECG or why your patient is getting heparin.
- Don’t worry about taking 9274748292 notes on rounds - usually it’s hell niche stuff, and not relevant. Maybe just a few key words
- Writing in notes: This is super daunting, especially when you aren't sure of what is going on. The best thing to do if after a ward round/when thing are quieter - ask one of the interns to show you how to write notes properly. It is an important skill to learn and practise early and is one of the ways you can contribute to the rounds.
- Clinical learning: I learnt this really late and it helped me a lot when it came to exams. Try and see at least one case (Hx and Exam) each day- this isn't possible all the time but strive for this. After you get home, read about this case presentation, possible differentials and red flags. Correlating a clinical case to theory is a fantastic way to make sure the information sticks.
What are some High Yield Education Activities?
Advice found in Orientation Document for Medical Students at Sir Charles Gairdner Hospital (Click for full document), compiled by Dr Christopher Ng, and reviewed by Dr Victor Yau and Dr Talia Shepherd.
- History taking and examination of patients in the Emergency Department with the admitting Surgical Admission Unit (SAU) registrar
- Being quizzed on how to interpret diagnostic tests and how to manage patients by any of the team members
- Insertion of IV cannula under aseptic techniques
- Taking bloods/venepuncture
- Going to surgical department clinics and sitting in with the consultants/fellows/registrar
- Observing or Scrubbing in for procedures (that you are interested in) in the operating theatres
- Going to teaching or tutorial sessions
- Attending multidisciplinary team meetings
- History taking and examination of patients independently on the ward, then presenting them to the team registrars or any team members
Please review this set of GeekyMedics videos to brush up on your examination skills prior to the rotation:
Please review this set of GeekyMedics videos before attempting any procedure on real patients:
How do I learn to use all of the online systems within the hospitals?
- Grab the intern/RMO after rounds or whenever they look not super busy and ask them to help you set up a list on day 1.
- Honestly, the interns are your best friends in regard to this. To get you started, here is a quick guide:
- Isoft: Ward lists, Pathology results, Patient lists
- Ask someone to show you how to access discharge summaries. These are super helpful for assignments ep operation report on surg.
- IMPAX: Radiology images and reports, Imaging
- This isn’t available to students and our HE number won’t work on here so you will have to find alternative logins from the interns or upper years (shhhhh).
- TMS: Theatre management system
- This is your best friend on a busy surgery team because you can see which surgeon is operating on who, what the surgery is and what theatre they are in.
- BossNet: Available at FSH, Fremantle and a few of the regional hospitals.
- This is the future and is the online notes management system. These hospitals have portable computers for the interns to take notes on and they are uploaded to boss net. If you are at other hospitals then you try read the Doc’s handwriting (good luck).
- Isoft: Ward lists, Pathology results, Patient lists
How can I be most helpful to the team?
- It’s hard to be useful most of the time but they will appreciate the effort. Little things like keeping path and radiology forms in your nerd box can be helpful.
They can also be found on the Department of Health, Government of Western Australia website
How should I take notes?
Advice found in Orientation Document for Medical Students at Sir Charles Gairdner Hospital (Click for full document), compiled by Dr Christopher Ng, and reviewed by Dr Victor Yau and Dr Talia Shepherd.
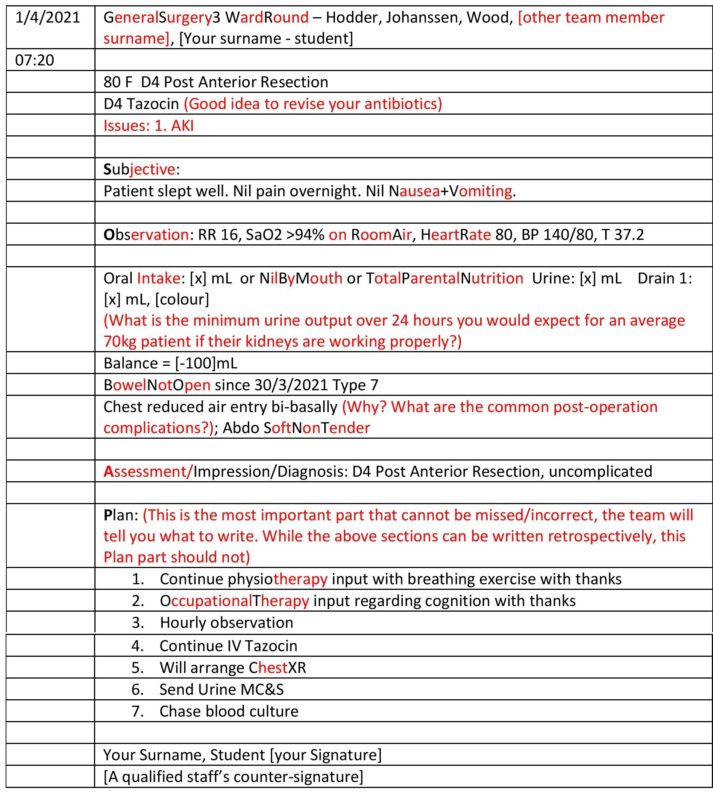
You are expected to arrive 10 minutes before the start of each ward round every day. When you arrive at the ward, bring your smile alongside with the patient’s medical files. You are expected to collect all the patient’s medical files so that you don’t have to run around to find them during the ward round. Surgical Ward are brief and succinct so that the consultants, fellows & registrars can attend Theatre team meeting on time.
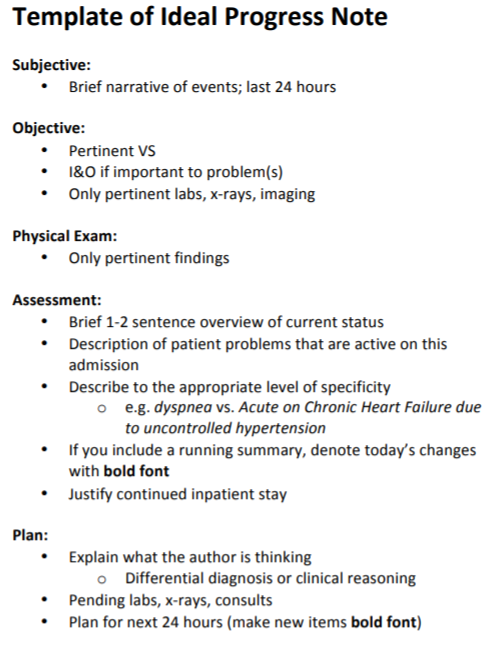
Most inpatient progress notes follow the format of SOAP (Subjective, Observations, Assessment, and Plan).
More from WAMSS Clinical Preparation Workshop. More from Geeky Medics.
Your job as a student includes proper documentation as per the following example:
Inpatient Progress Notes
What do I do if I feel like I’m not getting adequate teaching?
- Junior doctors rotate frequently at hospitals and teams frequently change, but sometimes, your experience is affected by the culture/environment of one particular site.
- If you did not have a good experience, It is very helpful if you tell someone about this; ideally your Discipline Coordinator who is responsible for organising placements at each site. They are best placed to action feedback.
- You can do this by directly emailing them (the email is in the Unit Guidebook) (please cc your year reps – this helps year reps better represent your cohort, and also helps to follow up on your feedback the next time they attend a Year Committee meeting.)
- If you don’t want to contact them yourself directly, again, please tell your year reps. You also get end of rotation surveys. There have been concerns that these are not anonymous and that you get chased up if you say rude things. These comments are largely reviewed at the end of the year in bulk rather than after each individual rotation in order to preserve anonymity. It also means that there is a delay in implementing the changes of these surveys, so better if you just tell someone about it!
How long do I have to be at the hospital for?
- You are expected to be there for ward rounds (especially for consultant ward rounds, don’t miss those!). As I said above, if you are offered to go to a clinic etc, you should really go.
- Some teams are more hectic than others. If you find that you are there a lot then I would be looking at discussing this with your team and tell them that you need more time to study.
- Stick around and leave when it’s reasonable - this means not to disappear without telling anyone, because that’s the actual worse (in my opinion). If you don’t feel like you’re getting much out of your attendance, talk to someone about it before leaving to study on your own.
- Sometimes, you have to stay the whole day just to get in the consultant's good books even though the learning may not be super valuable. If you make a good impression at the start, it may get easier to slide away later.
- Don’t try to pretend you get all Friday afternoons off for scholarly - you never really do - soz*
- If you want to stay longer - be honest about it
What if I get in the way?
- Getting in the way: You will ALWAYS be in the way, that is what medical students are for. That doesn't go away until after you graduate so just come to terms with it. It's not you, it's the system.
How did you feel when you first entered the wards and how did you overcome these feelings?
- How did I first feel? Awkward AF. The best thing to do on your first day is to introduce yourself to the ward clerk (just look for someone on the front computer at the nursing station). Tell them who you are and what team you have been assigned to and they will tell you where to wait for the team. I found the first thing that the registrar or consultant will ask you when you arrive is, “what do you have to get out of this rotation.” This is super vague and is always met with blank stares. Remember, you are primarily there to learn rotation specific history, examination and presentation skills as well as meet your core conditions. The best way to overcome feeling awkward is to come across as enthusiastic. The team will see that and try and get you involved as much as possible.
- Hot hint: if one of the doctors offers you teaching or asks if you want to come to the clinic – DO IT. It looks super bad if you decline their offer to go home (unless it is an unreasonable request). The consultants literally get nothing out of you being there so if they are offering you these opportunities then take them up on it and you will be given more chances to do cool stuff in the future.
What do I wear on ward rounds?
- Shoulders covered, nothing too tight.
- Pants are good because pockets, but skirts are fine as long as not too short.
- Generally, hair longer than shoulders needs to be up but depends where you are, on geris no one minded.
- Shoes: nice shoes that are enclosed. Eg brogues/oxfords, ankle boots, can maybe get away
with flats. I wear my rollies everyday (check gumtree etc for cheaper ones!) they are super comfy. - The rule is bare below elbows but sometimes you can wear a watch. Stud earrings, a small necklace.
- Don’t stress about having heaps of different outfits, all you really need is a couple pairs of pants/skirts and a few tops. It’s so fine to repeat outfits!
- Dudes: long pants (chinos are fine), belt, an ironed shirt (seriously, iron your shirt).
How do I know what to study?
- I found it really hard to study during the clinical year – would come home from prac and last thing I would want to do is study. But closer to exams its important you have an understanding of core conditions – but the exam is very clinical based so being on the ward and seeing how you treat a patient will help. Feel like you know nothing all year and then eventually it starts to click (somewhat). Oxford clinical cases is an excellent book – if you do nothing – read this before exams!!!!!
- Year 2 -? Pt presents with X - what makes diagnosis Y more likely diagnosis Z.? What on examination points to diagnosis Y and what points to diagnosis Z.? Medications for diagnoses GP CBLs and Multi-disciplinary seminars are examinable content!
- One thing I wish I got told a bit earlier was that centralised teaching is the most examinable fair game content of all time. Don’t mess around or skip your GP teaching and seminars. GP is equally weighted with all your other rotations and the questions are the most predictable.
- Towards exams, go through oxford clinical cases with a group of mates. Great for page turner exam.
How should I address Assessments?
- Get used to not caring too much about marks. It’s very subjective and each doctor will mark differently. Some doctors will think a 10/10 is standard of an intern, others will say it’s a good MD2. Expect lots of 6.5s. Ask for feedback and use that as your performance indicator – the marks don’t mean much and will weigh each other out by the end of the year! Learn things that will make you a good doctor, not give you good marks – that’s what matters at the end of the day.
Where can I get help?
If you’re feeling bullied, stressed or burnt out:
- Get a GP. Do it anyway. Visit them once every 3-6 months, even if you’re good.
- Check out the WAMSS Bullying guide.
- Talk to the unit coordinator or your supervisor.
- Check out our Humans of Medicine series, where doctors share personal stories about their journey through medicine.
Do I need to network / do research?
- You all probably want to get into a speciality which is increasingly competitive and have heard that ‘yOu NeEd tO sTaRT dOiNG rEsEArCH aS a StUDeNT oR yoU Won’T gEt iN’. Reality is, many junior doctors don’t even know what they want to do and haven’t started research or masters in their dream field.
- If you really want to start planning (which is fine – I did it) – talk to the reg or fellow on the team about whether they have any contacts. If you’re on placement in a field you want to do, ask the consultant whether you can help with any research projects they have going on, or whether you can do your elective with them eventually.
Hospital Guides?
- Specific hospital guides can be found in the (MD2-4) folder of WAMSS Notes.
- RCS Site Cheat Sheet can be found in the MD2 folder of WAMSS notes.
- As well as this, our RCS Representative can be contacted at [email protected]
Continue to the next page